Many women come to us thinking something is "off with their hormones"; and while that absolutely could be true, oftentimes the gut could be at play as well. Your gut is the upstream system that decides how estrogen gets recycled, how cortisol responds to stress, how thyroid hormone gets converted, and how progesterone is metabolized. That's why so many women optimize their hormones and still don't feel right. That's why we normally recommend a GI-Map as the test to run first, with a DUTCH right after or alongside it.
Almost every woman in her 30s or 40s has had this conversation with herself.
Something is off. PMS is different. Sleep is worse. Skin is changing. Mood is shorter. Body composition is harder. It must be my hormones.
She's not wrong. Hormones are real. They shift with age, with motherhood, with stress, with the years a woman has been running on too little sleep. Hormone testing is a meaningful piece of a real workup, and it's why we use the DUTCH at SeshDx alongside the GI-Map.
But "it's my hormones" is rarely the whole answer. More often, it's the visible end of a longer chain, and the start of that chain is the gut.
Your hormones aren't lying. They're just downstream.
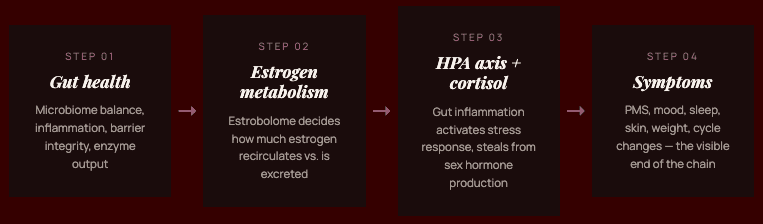
The gut isn't separate from your hormonal system. It is, in several measurable ways, part of it.
The estrobolome — a specific group of gut bacteria — produces an enzyme called β-glucuronidase that decides how much estrogen gets recycled back into circulation versus excreted. About 20% of T4-to-T3 thyroid conversion happens in the gut, dependent on a healthy microbiome. Gut inflammation activates the HPA axis (your stress system), which steals raw materials from sex hormone production and shunts them toward cortisol. And gut bacteria produce, degrade, and modulate histamine, which estrogen amplifies and which drives a surprising number of cycle-related symptoms.
In other words: when your gut goes sideways, your hormones follow. Test the hormones and you'll see the consequence. Test the gut and you'll see the cause.
The estrobolome: the gut bacteria that run your estrogen
If you only learn one piece of physiology from this post, learn this one.
After your liver processes estrogen for excretion, it sends the metabolites to your gut to leave the body. The estrobolome can either let that estrogen leave or reactivate it and send it back into circulation.
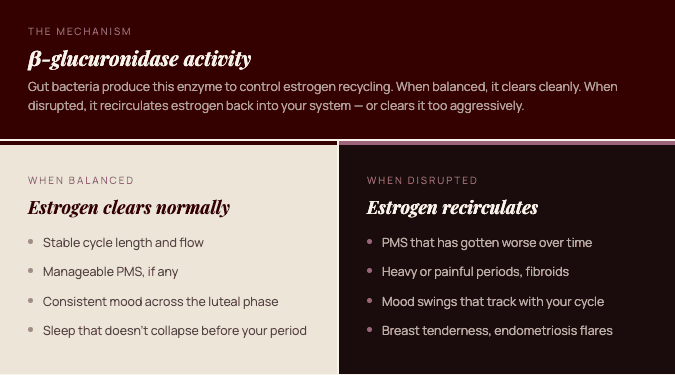
When the estrobolome is balanced, estrogen levels stay where they should. When it's dysregulated:
Too much β-glucuronidase activity → too much estrogen reabsorbed → PMS, breast tenderness, heavy or painful periods, fibroids, endometriosis flares, "estrogen dominance" symptoms
Disrupted gut function generally → erratic estrogen clearance → unpredictable cycles, mood swings, sleep disruption that tracks with your cycle
A DUTCH test will show you elevated estrogen or off-pattern metabolites. A GI-Map will tell you whether your gut is why.
How gut dysfunction creates "hormonal" symptoms
Here's where the gut actually drives the experience women associate with hormones:
PMS that's gotten worse. β-glucuronidase activity is one of the most under-appreciated drivers of premenstrual symptoms. When your gut is recirculating estrogen aggressively, the luteal phase hits harder.
Heavy or painful periods. Same mechanism. Excess circulating estrogen, often layered on top of gut-driven inflammation, intensifies bleeding and cramping.
Mood swings around your cycle. Gut bacteria produce GABA, dopamine, and serotonin precursors. Cyclical hormonal shifts that should feel manageable feel intolerable when the underlying neurotransmitter buffer is depleted.
Sleep disruption in the luteal phase. Progesterone supports sleep, but its action depends on adequate GABA and a calm HPA axis. Gut inflammation drives both in the wrong direction. This is why sleep gets worse the week before your period even when progesterone is technically "fine."
Fatigue and brain fog that track with your cycle. Cyclical fluctuations in immune signaling and inflammation amplify gut-mediated brain fog. The hormones changed; the gut decided how loudly the body would feel it.
Stubborn weight despite hormone optimization. Insulin sensitivity, GLP-1 production, and cortisol response are all gut-mediated. Optimizing hormones without addressing the gut is like tuning the dashboard while ignoring the engine.
Histamine reactions that come and go with your cycle. Estrogen amplifies histamine, and gut bacteria produce and degrade it. Cycle-triggered histamine reactions like flushing, headaches, anxiety spikes, food intolerances usually trace back to gut.
When it really is "just" hormones
This is the part most gut-health content skips, and we won't.
Sometimes the primary issue is hormonal. Perimenopause and menopause are real and measurable. Severe PCOS, thyroid disease, fertility challenges, and endocrine disorders deserve direct hormonal evaluation and, often, hormonal intervention. A woman in her late 40s with vasomotor symptoms and a clinical estrogen drop is not a gut-first case.
But even in those cases, gut function determines how well the hormonal intervention works. Estrogen replacement only works as well as the gut clears the metabolites. Thyroid medication only works as well as the gut converts T4 to T3. Cortisol regulation only works as well as the gut isn't driving systemic inflammation.
The gut is rarely the whole story. It's almost always part of it.
The right order to test
If we had to choose one place to start with most women presenting with hormonal complaints, it would be the GI-Map. Not because hormones don't matter, but because:
The gut is upstream. Fix the gut and many "hormonal" symptoms resolve without ever touching a hormone protocol.
Hormone interventions work better. When the gut is functioning, every downstream hormonal therapy (bioidenticals, thyroid medication, supplements) performs closer to its potential.
The mechanisms are visible on a stool test. β-glucuronidase, dysbiosis, inflammation, intestinal permeability, digestive function — all the gut-side hormonal levers show up on the GI-Map.
For most women, the highest-leverage starting point is a GI-Map alone. For women with cycle disorders, perimenopausal symptoms, suspected thyroid involvement, or a history of birth control / IUD use, we typically pair it with a DUTCH.
What the GI-Map shows that a hormone test doesn't
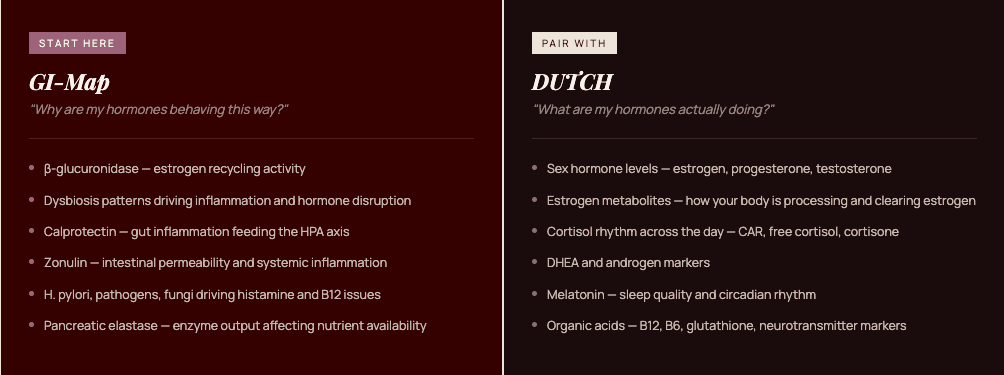
A hormone panel tells you the what. A stool test tells you the why. Specifically, the GI-Map quantifies:
β-glucuronidase activity — the estrobolome marker that drives estrogen recirculation
Dysbiosis patterns — which bacterial imbalances are present and how they map to symptoms
Pancreatic elastase — digestive enzyme output, which collapses under chronic stress and drives nutrient shortfalls that affect hormone production
Calprotectin — gut inflammation, which feeds the HPA axis and skews cortisol
Zonulin — intestinal permeability, the lever behind food sensitivities and systemic inflammation
Pathogens, parasites, fungi — including H. pylori, which drives histamine and B12 issues that masquerade as hormonal
Anti-gliadin IgA — gluten reactivity, which independently disrupts thyroid function and inflammation
A DUTCH will show you what your hormones are doing. A GI-Map will tell you why.
The bottom line
Your hormones aren't lying. They are responding to inputs upstream of them. For most women in their 30s and 40s, the loudest of those inputs is the gut.
You don't have to choose between testing your hormones and testing your gut. You just have to test in the right order — and the gut is usually it.
Find out what's actually driving your hormonal symptoms.
Pair it with the DUTCH Complete Hormones + Cortisol test if you want the full hormonal picture. Our team interprets both, together, and builds your protocol from the upstream cause.
Frequently asked questions
How do I know if my symptoms are hormonal or gut?
Most of the time it's both. Hormones reflect what your body is doing; gut health is one of the strongest determinants of why. Symptoms that track tightly with your cycle, started after antibiotics, or worsen with stress and food are particularly likely to be gut-mediated even when they look hormonal.
Should I get a hormone test or a stool test first?
For most women in their 30s and 40s, a GI-Map is the highest-leverage starting point because the gut is upstream of the hormonal system. We often pair it with a DUTCH for cycle disorders, perimenopause, suspected thyroid involvement, or a history of hormonal birth control.
Can fixing my gut actually fix hormonal symptoms?
For many women, yes. β-glucuronidase activity, gut inflammation, dysbiosis, and intestinal permeability are direct levers on estrogen, progesterone, cortisol, and thyroid function. Resolving them often resolves the symptoms women had attributed to hormones.
What is the estrobolome?
The estrobolome is the collection of gut bacteria that metabolize estrogen via the enzyme β-glucuronidase. It controls how much estrogen gets recycled back into circulation versus excreted, and it's one of the most under-recognized drivers of estrogen-pattern symptoms.
Does perimenopause mean my problem is hormonal, not gut?
Not exclusively. Perimenopause is a real hormonal transition, but gut function determines how the body buffers it. Women who enter perimenopause with a healthy gut tend to experience the transition with fewer and less intense symptoms.
Will a GI-Map show hormone levels?
No — for that you need a DUTCH or other hormone panel. The GI-Map shows the gut-side mechanisms (especially β-glucuronidase, dysbiosis, inflammation) that influence hormone metabolism. The two tests are complementary.